-
Type:
Hosp Inpt eCQMs - Hospital Inpatient eCQMs
-
Resolution: Answered
-
Priority:
 High
High
-
Component/s: None
-
None
-
-
CMS0334v6, CMS1028v3
-
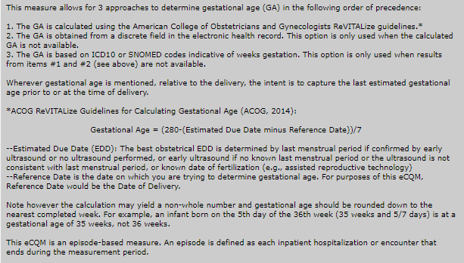
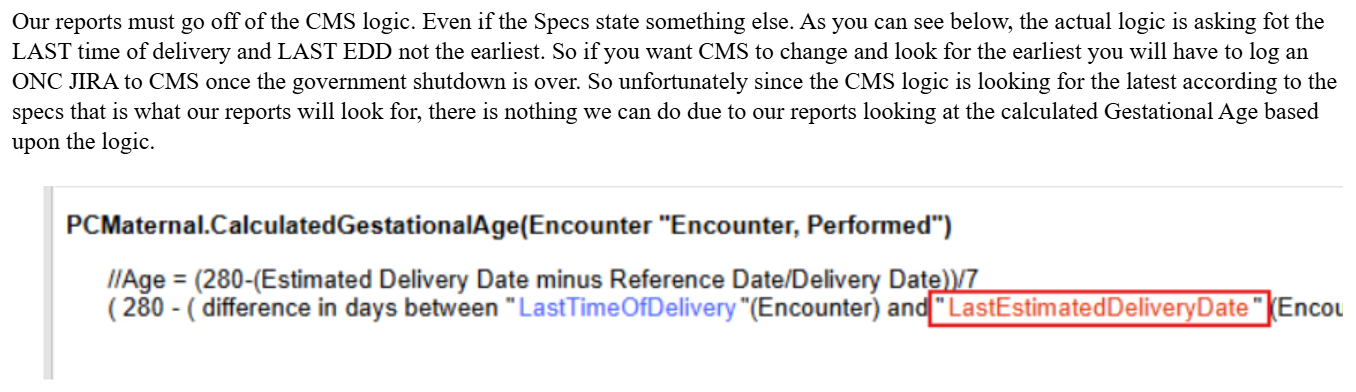
Previously our EDD wasn't pulling in and we were basing our gestational age at delivery by the 2nd method, by last EGA at delivery, which worked well enough. We recently took a new package from our vendor, and now the most recently documented EDD is pulling into the chart and calculating the gestational age at delivery. The trouble is, it's taking the most recent EDD, which is often not the most accurate EDD. The specs state that EDD should be determined by LMP and/or early ultrasound, which is how we practice clinically. However, every time the patient gets an ultrasound a new EDD is created in her electronic chart based on that ultrasound. In our EHR (Cerner) the pregnancy's EGA is always calculated off of the "authoritative" EDD. So all the EDDs from any ultrasounds and the LMP will be visible, but one is marked as "authoritative" and that's the official one. This is done by the provider per ACOG guidance on LMP and early ultrasound. Our vendor is saying that per the CMS logic, they have to take the "last" EDD, or the most recently generated EDD, not the "authoritative" EDD. So if the patient had a 20-week anatomy ultrasound, which most of them do, or an ultrasound even further along in the pregnancy, it's pulling that EDD, not the EDD from early in the pregnancy or from the LMP. It's not uncommon for the EDD to be off enough to bump the pregnancy along or behind a week or even 2 from what the early ultrasound EDD was. This is clearly contrary to the guidance in the specs, but the logic trumps the specs and the vendor says they are pulling the EDD correctly and there is nothing they can do to change it. Is this a correct interpretation of the logic?
{kind=link}