-
Type:
EC eCQMs - Eligible Clinicians
-
Resolution: Answered
-
Priority:
 Moderate
Moderate
-
Component/s: None
-
None
-
-
CMS0002v14
-
CMS0002v13
-
If just the procedure of performing the screening can qualify a patient for the denominator and does not require any additional coding this can increase the number of patients being screened in the denominator.
For the CMS2 measure, I am looking for clarification on the logic of the measure.
There are three Encounters, Performed for this measure.
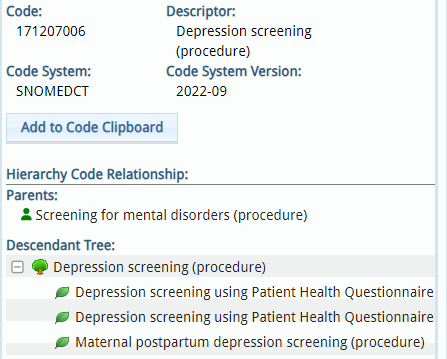
Under the ["Encounter, Performed": "Encounter to Screen for Depression"] Value Set there are 106 CPT, HCPCS, and SNOMED CT codes. When I look at that list I see SNOMEDCT 171207006 is Depression screening (procedure).
I then open up the Hierarchy Code Relationship and it includes depression screening using PHQ-2, PHQ-9 or Maternal postpartum depression screening.
I am wondering if a patient is screened using the PHQ-2 or -9, does that need to be tied to any specific CPT, ICD or other type of billing code to be a qualifying encounter? Or even if the patient is screened using the PHQ-2 but the encounter has a CPT code of 99211 (as opposed to 99212 in the ["Encounter, Performed": "Encounter to Screen for Depression"] Value Set) should that encounter still count as a qualifying encounter for the numerator of the measure?
Our EHR vendor has tied the SNOMEDCT 171207006 to the ICD-10 code "Z13.31 Encounter for screening for depression" and are claiming that we must have that ICD-10 code for the SNOMEDCT 171207006 code to count for the "Encounter, Performed". They are claiming that there is some other joiner or 'and' function that must be used to use that SNOMEDCT 171207006 "Encounter to Screen for Depression". Perhaps you can also clarify what is meant to occur for that SNOMEDCT "Encounter to Screen for Depression" to result in a positive function for patients to count in the denominator?