-
Type:
EC eCQMs - Eligible Clinicians
-
Resolution: Answered
-
Priority:
 Moderate
Moderate
-
Component/s: None
-
None
-
-
CMS0135v11, CMS0144v11, CMS0145v11
-
We are not meeting the case requirements for any of the LVSD measures due to conflicting ICD-10 requirements. There are only two ICD codes that describe 'moderate' or 'severe' LVSD and our coders do not like either of them.
I need some guidance/clarification on the LVSD (LVEF >40%) measures. I work in a cardiology specialty. We are struggling to meet the minimum case requirement for the LVSD clinical quality measures, and I think it is because the CMS wording may be outdated. I do not intend to sound brash; if this is not the case, I would greatly appreciate any guidance. We want to participate in the MVPs this year and need to understand these measures and their requirements fully. We use EPIC as our CEHRT.
CMS 145
In 2022, we had over 7300 people in the initial population. We had zero issues with this measure's 145.2 - 'Prior MI' portion (over 1200 in the numerator with a 96-98% performance rate). However, we only had thirteen patients in the denominator of the 145.1 - LVSD (LVEF >40%). This measure consists of the same initial population.
CMS 144
Same issue. Only thirteen patients showed a moderate or severe LVSD diagnosis.
CMS 135
Same issue.
I audited over 500 patients last year. The thirteen patients in the LVSD measures had one of two diagnoses in common, I51.9.
Moderate left ventricular systolic dysfunction
SNOMED Code: 981000124106
Severe left ventricular systolic dysfunction
SNOMED Code: 991000124109
These two diagnoses are the only ones that explicitly state "moderate" or "severe" LVSD, and as I said, the only ones in the numerator. However, our billing and coding team state that I51.9 would never be sufficient for a primary billing diagnosis and does not want them listed as such. Our CMO, who is also the medical director of our heart (failure) improvement program, wants our providers to use the reduced or preserved ICD-10 diagnosis codes when documenting heart failure:
I50.30 - (HFpEF) heart failure with preserved ejection fraction (CMS/HCC)
- I understand this measure would not be intended for moderate or severe LVSD and would not apply to any of these measures.
I50.23 - Systolic heart failure with reduced ejection fraction (acute/chronic/acute on chronic)
This diagnosis does not indicate moderate or severe LVSD, so it is not satisfying the LVSD measures. However:
- "Reduced" ejection fraction is typically considered when a patient has an EF of less than 40%.
- An EF between 30-39% is moderately reduced
- An EF below 30 is severely reduced.
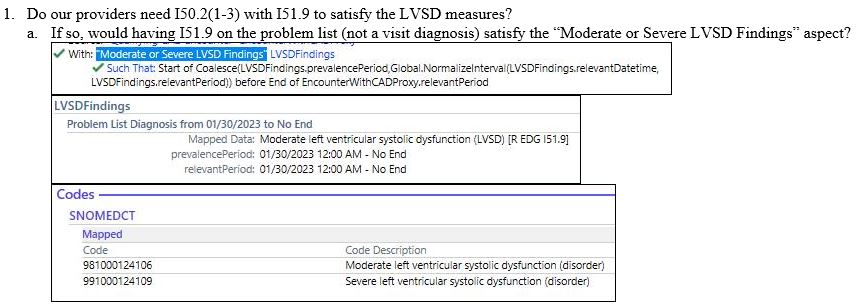
- Do our providers need I50.2(1-3) with I51.9 to satisfy the LVSD measures?
- If so, would having I51.9 on the problem list (not a visit diagnosis) satisfy the "Moderate or Severe LVSD Findings" aspect?
- Are there other ICD-10 codes we could/should be using that better suit the billing/coding aspect and meet the LVSD measures?
I look forward to your response and greatly appreciate the help. If I can provide more information, please do not hesitate to let me know.
Thank you again,
Michael Trager MHA, CMA
Clinical Improvement Consultant
1600 S 48th St., Suite 600
Lincoln, NE 68506
Tel: 402-483-3339