Hide
In the gray section of the specifications, the "Denominator" section reads, "Inpatient hospitalizations for patients with a principal diagnosis of ischemic stroke, and a history of atrial ablation, or current or history of atrial fibrillation/flutter." The CQL "Denominator" section states, "Encounter with Atrial Ablation Procedure".
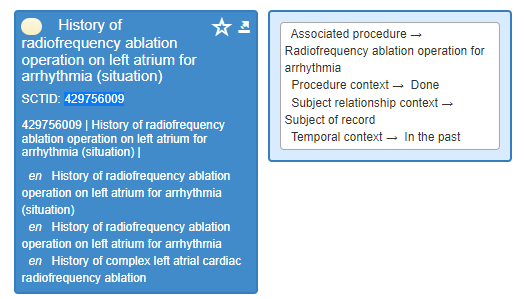
I had a chart that had a SNOMED Code for history of ablation, it was not a procedure code, but it was a code for "h/o ablation," which means that it happened prior. In the gray section of the specifications for the denominator, it does not say a history of atrial ablation "procedure", it simply says, "a history of atrial ablation".
Am I reading this correctly, that the history of atrial ablation SNOMED codes are not included, just procedure? If so, my question is, in the future, should SNOMED codes for "history of atrial ablation" be added, and not just procedure codes for atrial ablation?
This is quite confusing. It seems that based on the definition of the eSTK-3 Denominator, the measure should include all "history of," not just procedures. The patient could have had the "procedure" at an outside hospital and then the provider just documents "history of" at our hospital, to me this would still count.
Thanks!
Show
In the gray section of the specifications, the "Denominator" section reads, "Inpatient hospitalizations for patients with a principal diagnosis of ischemic stroke, and a history of atrial ablation, or current or history of atrial fibrillation/flutter." The CQL "Denominator" section states, "Encounter with Atrial Ablation Procedure".
I had a chart that had a SNOMED Code for history of ablation, it was not a procedure code, but it was a code for "h/o ablation," which means that it happened prior. In the gray section of the specifications for the denominator, it does not say a history of atrial ablation "procedure", it simply says, "a history of atrial ablation".
Am I reading this correctly, that the history of atrial ablation SNOMED codes are not included, just procedure? If so, my question is, in the future, should SNOMED codes for "history of atrial ablation" be added, and not just procedure codes for atrial ablation?
This is quite confusing. It seems that based on the definition of the eSTK-3 Denominator, the measure should include all "history of," not just procedures. The patient could have had the "procedure" at an outside hospital and then the provider just documents "history of" at our hospital, to me this would still count.
Thanks!
Hosp Inpt eCQMs - Hospital Inpatient eCQMs
 Moderate
Moderate

Joelencia Leflore
Rebecca A John